


1Department of Dermatology, Huashan Hospital, Fudan University, and 2Children’s Hospital & Institutes of Biomedical Sciences, Fudan University, Shanghai, China
DRESS is one of the most severe drug reactions. The aim of this retrospective study was to summarize the clinical presentation, genetic predisposition and prognostic factors of DRESS. A total of 52 patients with DRESS, who were inpatients at a medical referral centre in Shanghai, China, from January 2011 to December 2016, were analysed retrospectively. All the patients had skin eruption, 83% had liver involvement, and ≤10% had other organ involvement. Mean cost of hospitalization was US$5,511 ± 3,050. The 3 most common causative agents were allopurinol (18/52; 35%), salazosulphapyridine (11/52; 21%) and carbamazepine (5/52; 10%). HLA-B*5801 and HLA-B*1302 were associated with allopurinol-induced DRESS. HLA-B*1301 was related to salazosulphapyridine-induced DRESS. The mortality rate was 6% (3/52). Epstein-Barr virus DNA was found in 10 patients (19%) and indicated a poor prognosis. Human herpes virus 6 DNA was detected in 17 patients (33%) and was associated with autoimmune sequelae. Due to its high medical cost and sometimes poor prognosis, prevention of DRESS should be a high priority.
Key words: drug reaction with eosinophilia and systemic symptoms; drug hypersensitivity; adverse drug reaction; human herpes virus; human leukocyte antigen.
Accepted Dec 14, 2017; Epub ahead of print Dec 15, 2017
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Xiaoqun Luo, Department of Dermatology, Huashan Hospital, Fudan University, Shanghai 200040, China. E-mail: luoxiaoqun913@126.com
Drug reaction with eosinophilia and systemic symptoms (DRESS), or drug-induced hypersensitivity syndrome (DIHS), ranks among the most severe cutaneous drug reactions and may be life-threatening. Apart from extreme eosinophilia and organ dysfunction, its characteristics include a long latent period, fever, skin rash and lymphadenopathy. Because of its complex natural course and various clinical manifestations, it is difficult to make a diagnosis of DRESS. In 2007, the European registry of severe cutaneous adverse reactions (RegiSCAR) established the diagnostic criteria for DRESS (1) and thus clarified the definition.
During the past decade, numerous studies have reported genetic predispositions of severe cutaneous adverse reactions (SCARs). Correlations between multiple human leukocyte antigen (HLA) alleles with specific drug-induced SCARs have been identified (2). For example, HLA-B*5801 has a strong correlation with allopurinol (ALP)-induced SCARs in Thai and Han Chinese populations (3, 4). The negative predictive value of HLA-B*5801 was high, although its positive predictive value was comparatively low (3, 5). This means that many ALP-tolerant patients also carry this allele. Moreover, very few studies have analysed the associations between HLA alleles and each subtype of SCARs. Due to its low incidence, a large population analysis concerning the association between the HLA allele and DRESS is currently lacking.
Apart from genetic predisposition, reactivation of the human herpes virus (HHV) family also plays a key part in the pathogenesis of DRESS. However, the role of the HHV family is controversial. Some authors report that DRESS is the consequence of viral reactivation (6), while others regard these infections as complications of immunosuppressive therapy (7). Previous studies have observed an association between HHV6 reactivation and the severity of DRESS (8, 9). However, the role of virus reactivation in the natural chronic course of DRESS and in relapses remains hypothetical (10). Large-scale retrospective studies analysing the relationship between HHV reactivation and the prognosis of DRESS are limited.
The aim of the current study was to analyse the most common culprit drugs, latent period and medical cost of Chinese patients with DRESS. Particular attention was paid to the genetic predisposition and prognostic factors of DRESS.
Medical records of all patients hospitalized in the Department of Dermatology at Huashan Hospital affiliated to Fudan University in Shanghai, China between January 2011 and December 2016 were retrospectively reviewed. Patients diagnosed with “drug eruption” and “drug hypersensitivity syndrome” were listed as suspected DRESS patients. These patients’ whole-blood samples were prospectively collected within 2 days after admission unless otherwise indicated. Follow-up was accomplished via a phone interview. All patients were followed up for at least 6 month after discharge.
According to RegiSCAR diagnostic criteria, patients with suspected DRESS were classified as de?nite, probable, possible, or no case. Those whose final points failed to reach 2 (defined as no case by RegiSCAR diagnostic criteria) were excluded from the study.
Two control groups were recruited in this study. The first control group was chosen from the human MHC database (dbMHC) (11). It consisted of 283 unrelated healthy Chinese people. The other control group consisted of patients who did not develop any cutaneous eruptions after being treated with ALP or salazosulphapyridine (SASP) for more than 3 months (i.e. ALP-tolerant and SASP-tolerant group). The second control group was recruited from the Department of Rheumatology of Huashan Hospital. The ethics committee of Fudan University approved the study. Informed consent was provided by each participant. Patients in the control groups were all Han Chinese.
Eosinophilia was diagnosed when absolute eosinophil counts exceeded 700/μl. If the total leukocyte count was less than 4,000/μl, it was considered when the percentage of eosinophils surpassed 10%. A high level of serum IgE (sIgE) was defined as sIgE exceeding 240 ng/ml. Hepatic damage was considered when the level of serum alanine aminotransferase (ALT) exceeded twice the normal limit, or 2 times the patients’ baseline levels. Renal damage was defined as the level of serum creatinine exceeding twice the normal values or when the patient developed recent onset of haematuria or proteinuria. Cardio-muscular and pancreatic involvement were considered when the patient’s cardiac or muscular enzymes or amylase levels exceeded the normal range. Culprit drugs were identified by the criteria proposed by Naranjo et al. (12).
QIAamp DNA Blood mini kit (Qiagen Inc., Valencia, CA, USA) was used to extract genomic DNA from peripheral blood samples. LABT® SSO Kit (One Lambda, CA, USA) was used to detect HLA-A, -B and -C alleles by PCR sequencing of specific oligonucleotides. All genotypings were reanalysed by HLA Fusion™ software, version 3.0 (One Lambda, CA, USA). Mentality Bio-Tech Co. Ltd (China) helped with the genotyping.
Taqman real-time PCR procedure was used to amplify and quantify respectively the EBV and HHV6 gene region from the DNA sample. EBV and HHV6 reactivations were defined as quantity of DNA copies above the detection threshold (1×103 copies/ml).
Descriptive variables were listed as number (percentage) or mean ± standard deviation (SD) or median (range). Comparisons of the parametric data were performed using Student’s 2-tailed t-test. Non-parametric data were compared by χ2 square or Fisher’s exact test, if appropriate. A multivariate logistic regression was performed to eliminate the effects of confounding factors. Differences were regarded as significant when p < 0.05. Data were analysed with SPSS17.0 (SPSS Inc., Chicago, IL, USA).
Of all inpatients of the Dermatology Department at Huashan Hospital affiliated to Fudan University between January 2011 and December 2016, 52 were classified as DRESS patients and were enrolled in this study. Among them, 15 (29%) patients were classified as definite cases, 33 (63%) as probable cases, and 4 (8%) as possible cases by the RegiSCAR scoring system.
A total of 34 male patients and 18 female patients were enrolled. The male:female ratio was 1.88:1, and the median age was 47.5 years (range 20–81 years). Median latency time was 30 days (range 4–100 days). The mean length of stay was 13 ± 6 days. The mean cost of medicine to treat DRESS was US$4,091 ± 2,618 (¥26,749 ± 17,120). The mean hospitalization cost was US$5,511 ± 3,050 (¥35,938 ± 19,890). The 3 most common causative agents were ALP (18/52; 35%), SASP (11/52; 21%) and carbamazepine (CBZ, 5/52; 10%).
HLA alleles correlated strongly with ALP, SASP, and CBZ-induced DRESS by Fisher’s exact tests are listed in Table I. HLA genotypes of all 52 patients with DRESS, along with their general clinical characteristics, are available from the authors on request.
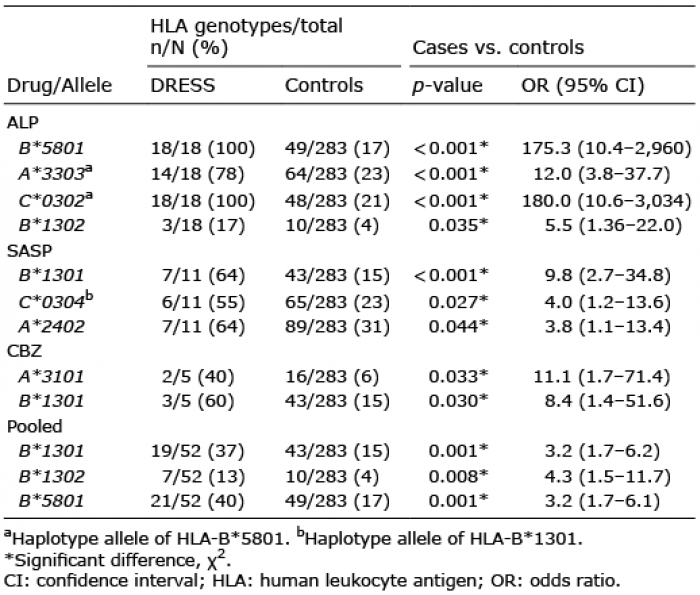
Table I. Genetic risk factors for allopurinol (ALP)-, salazosulphapyri-dine (SASP)-, and carbamazepine (CBZ)-induced drug reaction with eosinophilia and systemic symptoms (DRESS)
Four alleles were significantly associated with the ALP-induced DRESS group: HLA-B*5801, HLA-A*3303, HLA-C*0302 and HLA-B*1302. Because of the high co-appearance rate with HLA-B*5801: 76% (16/21) for HLA-A*3303 and 100% (21/21) for HLA-C*0302, these 2 alleles were regarded as haplotype alleles of HLA-B*5801 (13). Therefore, only HLA-B*5801 and HLA-B*1302 remained relevant. HLA-B*5801 was most closely related to ALP-induced DRESS (p < 0.001, odds ratio (OR) 175.3, 95% confidence interval (95% CI) 10.4–2,960.0).
In SASP-induced DRESS group, 3 alleles were found to be strongly correlated: HLA-B*1301, HLA-A*2402 and HLA-C*0304. The HLA-C*0304 allele is recognized as a haplotype allele of HLA-B*1301 (13), emerging along with HLA-B*1301 in 17 (89%) of 19 cases. Therefore, HLA-B*1301 was most closely related to SASP-induced DRESS (p < 0.001, OR 9.8, 95% CI 2.7–34.8).
In the CBZ-induced DRESS group, both HLA-A*3101(p = 0.033, OR 11.1, 95% CI 1.7–71.4) and HLA-B*1301(p = 0.030, OR 8.4, 95% CI 1.4–51.6) were associated.
Pooled analysis identified HLA-B*1301, HLA-B*1302 and HLA-B*5801 as independent risk factors to induce DRESS (Table I). The correlations remained significant after multivariate logistic regression to eliminate interactions between the alleles (Table II).
Table II. Comparison of human leukocyte antigen (HLA)-B*5801, HLA-B*1302, HLA-B*1301 in predicting drug reaction with eosinophilia and systemic symptoms (DRESS) (multivariate logistic regression)
All patients (n = 52) had skin eruption. Fever and lymphadenopathy were the other most common clinical manifestations, present in 39 (75%) and 36 (69%) patients, respectively. At least one internal organ involvement was observed in 48 (92%) patients. Liver damage was the most frequently observed (43/52; 83%). Other impaired organs included heart (3/52; 6%), pancreas (2/52; 4%) and kidney (2/52; 4%). Eosinophilia was present in 42 (81%) patients, 29 (56%) patients had high sIgE level. More than half of the patients with high sIgE level (52%) had values higher than 2,000 ng/ml. EBV reactivation was found in 10 (19%) patients, and HHV6 reactivation in 17 (33%) patients.
The culprit drug was discontinued in every patient. The longest duration until discontinuation was 4 months (in this case CBZ was the culprit drug, with a cumulative dose of 5,500 mg). All patients received systemic corticosteroid therapy. Additional intravenous immunoglobulin (IVIG) therapy for 3–5 days was given to patients with aggravating signs (exacerbation of skin eruptions, worsening of laboratory findings, or other complications) after the treatment by 1.5 mg/kg/day of methylprednisolone for 3–5 days. IVIG was given by continuous infusion to patients without severe renal or heart failure. Twenty (38%) patients received corticosteroid therapy alone and 32 (62%) patients received additional IVIG therapy.
In this study, 3 patients died of infection within 3 months post-discharge. The clinical features of deceased cases are available from the authors on request. One patient developed fulminant type 1 diabetes mellitus (FT1D) during her stay in hospital. She was still on insulin therapy despite cessation of systemic corticosteroids 4 months post-discharge. HLA-A*0203, HLA-A*2402, HLA-B*5801, HLA-B*4003, HLA-C*0302, HLA-C*0304 alleles were carried by this patient. Three patients (6%) developed hyper/hypothyroidism during follow-up (within 1 year post-discharge). Prior HHV-6 reactivations were detected in all 3 patients.
The reported incidence of DRESS varied from 1 in 10,000 to 1 in 1,000 drug exposures (14, 15). Despite the low incidence, DRESS is associated with high mortality, very high healthcare costs and chronic autoimmune sequelae (10). In this study, the mean hospitalization cost of DRESS is 164% of per capita disposable annual income in China (US$3,067 or ¥ 20,167) (16).
In accordance with previous pharmacogenetics research, HLA-B*5801 was strongly associated with ALP-induced DRESS in Han Chinese patients (4, 5). However, pretreatment screening of HLA-B*5801 alone might overestimate the risk as the ALP-tolerant population also carried HLA-B*5801, (7/63; 11%) in this study and 20/153 (15%) in other published data (5). As described in Table I, HLA-B*1302 was also related to ALP-induced DRESS. Moreover, none of the ALP-tolerant control carried HLA-B*1302 allele (Table III). Therefore, we speculate that HLA-B*1302 plays a complementary role in the pathogenesis of DRESS. Additional pretreatment screening of HLA-B*1302 could help physicians to choose ALP-tolerant patients from a HLA-B*5801-positive population.
Table III. Comparison of human leukocyte antigen (HLA)-B*5801 and HLA-B*1302 in predicting allopurinol-induced DRESS
SASP is frequently used to treat inflammatory colitis and ankylosing spondylitis. As previously reported by our research group (17), HLA-B*1301 was most closely associated with SASP-induced DRESS. In the SASP-tolerant group, the carrier frequency was 13% (4/30). The negative and positive predictive values were 0.87 (95% CI 0.69–0.96) and 0.64 (95% CI 0.31–0.89), respectively. HLA-B*1301 was also reported to be related to the dapsone hypersensitivity syndrome among patients with leprosy (18). The structural and metabolic similarity between dapsone and SASP might explain this overlap (19, 20).
In addition to genetic predisposition, reactivation of the HHV family also plays a role in the development of DRESS. HHV6 reactivation was found to be exclusive to DRESS, while reactivation of other HHV family members was observed in other SCARs (7, 21). In our series, interestingly, HHV6 was positive in all 3 patients who developed hyper/hypothyroidism during follow-up. The infection rate was significantly higher than those without autoimmune sequelae (p = 0.03, OR 17.14, 95% CI 0.83–353.40). In agreement with previous studies (22, 23), the high incidence suggested that chronic virus reactivation might have triggered excessive autoimmune responses and induced autoimmune diseases after DRESS remission. Another proof is the low incidence of autoimmune sequelae in SJS/TEN (24), during which viral reactivations were less frequently observed.
In this study, the mortality rate was 6% (3/52), consistent with reported mortality rate of DRESS (3–10%) (15, 25, 26). Multiple organ failure and sepsis were the main reported causes of death. No significant difference was found between patients receiving additional IVIG therapy and those without IVIG in terms of mortality (Table IV). IVIG has been widely used in SJS/TEN as it could block the Fas-Fas ligand interaction and thus prevent death of keratinocytes (27). Its use in patients with DRESS was suggested mainly because of its antiviral and immunomodulatory effects. In effect, experts have not yet reached consensus concerning the use of IVIG in patients with DRESS. One study found that the use of IVIG alone to treat patients with DRESS rendered poor benefit/risk balance (28). On the other hand, another consensus group suggested use of 2 g/kg/day IVIG for 5 days in association with corticosteroid to treat patients with life-threatening signs (29). Nevertheless, controlled clinical trials investigating the effectiveness and potential long-term complications of IVIG plus corticosteroid therapy for DRESS are currently lacking.
Table IV. Risk factors of death in patients with drug reaction with eosinophilia and systemic symptoms (DRESS)
EBV reactivation, detected in all 3 deceased patients, was associated with poor prognosis (Table IV). However, we could not perform multivariate logistic regression due to the limited number of deceased cases.
Due to the scarcity of DRESS, the number of patients included in our study was still limited. Furthermore, we only examined viral DNA on admission. A large-scale retrospective study concerning viral reactivation at different time-points of DRESS might be of greater interest.
In conclusion, we analysed the clinical features, HLA-genotypes and viral reactivation of 52 DRESS patients hospitalized in China during a 6-year period. Despite the heterogeneous clinical manifestations, DRESS represents a specific disease entity. High priority in public health and drug control agency should be given to the prevention of DRESS. HLA allele pretreatment screening, especially HLA-B*1301, HLA-B*1302 and HLA-B*5801 pretreatment screening, may help to prevent SASP and ALP-induced DRESS. EBV and HHV6 detections may predict the prognosis of patients with DRESS.
This work was supported by the National Natural Science Foundation of China (grants 81472873).
The authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize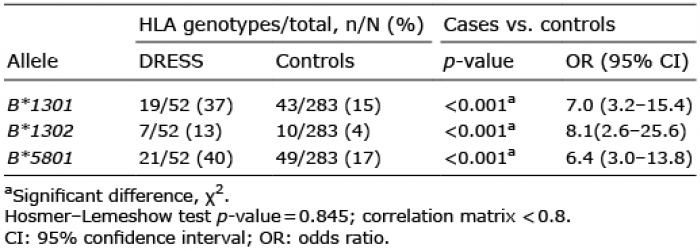 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize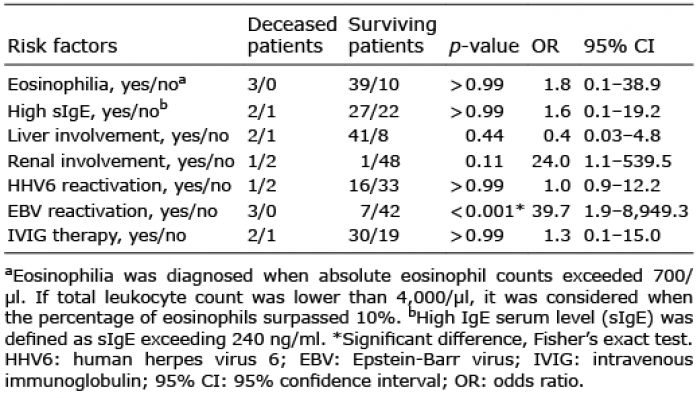 Click to show fullsize
Click to show fullsize